On Levodopa: How Does It Work?
Levodopa has been the primary treatment for Parkinson's disease for over half a century, and its ability to restore movement and how it works are unquestioned. When levodopa was initially approved by the FDA in 1970, there were a lot of unknowns about brain function in people with and without Parkinsons’s. The structure of dopamine receptors, the control of mitochondria, the impact of alpha-synuclein, the role of VMAT2 and relevance of apoptotic neuron death were unknown, as were their critical importance to the development, progression and impact of Parkinson’s.
In parallel, people tend to be surprised when I tell them I am not opposed to levodopa therapy at the same time I am advocating for reducing dopamine levels with RB-190.
But today, with the massive increase in knowledge since the 1960s, we now understand how levodopa works in Parkinson’s. I want to take you on a journey – with the risk of getting too technical – to share why the data say that levodopa's likely mechanism of action means its use can continue – with some guardrails – while we also pursue development of RB-190 as a dopamine reducing therapy to reverse Parkinson’s. While it may seem like a paradox, science defines how these two approaches can coexist.
The Standard Explanation for Levodopa’s Mechanism of Action
By the 1960s, we understood that movement was controlled by dopamine produced in the brain’s dopaminergic neurons. Studies showed that brain tissue dopamine levels were low in people with impaired movement. By treating these patients with levodopa, which is converted in the body to dopamine and therefore thought to replace the missing brain dopamine, movement was restored.
But if the disease were one of dopamine deficiency, then why does the effect wear off, eventually requiring higher doses?
The answer is connected to one of the key discoveries about Parkinson’s. The part of the brain containing dopaminergic neurons needs more energy to maintain normal function than just about any other part of the body. But in Parkinson’s, the microscopic “power plants” within the neurons – called mitochondria – do not work normally. These power plants produce only a fraction of what the brain cells needed. Thus, to understand levodopa’s mechanism of action in Parkinson’s we must consider the science in the context of cellular energy deficiency.
Based on today’s knowledge, let’s make a list of the steps required for levodopa to work as postulated in the 1960s, with each noted as whether independent or dependent on energy from the mitochondria.
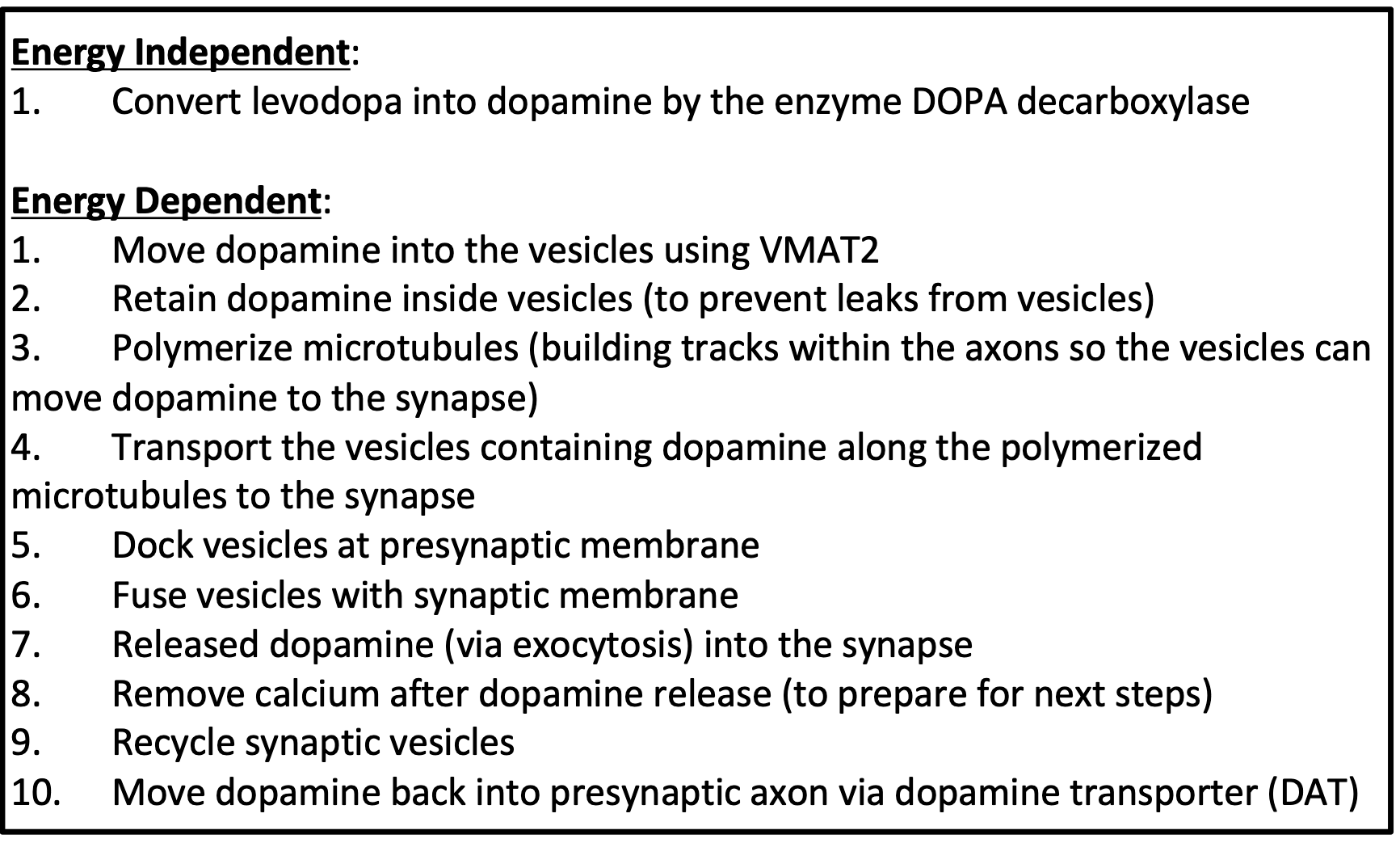
Only one of these critical steps is energy independent – able to work even with mitochondrial dysfunction and lack of energy in Parkinson’s disease.
With impaired energy production from the microscopic power plants, none of the energy dependent steps can happen efficiently when a person is affected by Parkinson’s. Recognizing the loss of power production means that the 1960s explanation for how levodopa works for people with Parkinson’s is not plausible.
To be clear, this knowledge doesn’t change levodopa’s unquestionable ability to improve movement, but it does question how levodopa is thought to work and taught since the 1960s and published in today’s textbooks.
What Does the Science Teach?
Two key scientific concepts establish the foundational insights: (1) availability of DOPA decarboxylase – the enzyme required to convert levodopa into dopamine, and (2) the intrinsic behavior of dopamine receptors – specifically how they respond to the stimuli that initiate and maintain normal movement.
In part due to the huge investment by the Michael J. Fox Foundation into a program called the Parkinson’s Progression Markers Initiative, we learned that the neurons of people with Parkinson’s leak the enzyme DOPA decarboxylase into the fluid surrounding the brain that in people without Parkinson’s is confined inside the dopaminergic neurons. The same DOPA decarboxylase in step 1 above is detectable in the fluid outside the neurons even in people who don’t yet have symptoms of Parkinson’s – referred to as prodromal disease.
With the enzyme DOPA decarboxylase in the extracellular fluid, treatment with levodopa produces dopamine outside the dopaminergic neurons, which then diffuses into the space between the dopaminergic neurons – the synapse. And because of the deficiency in energy, it stays there (because step 10 listed above doesn’t work properly without energy).
The dopamine receptors on the post-synaptic neuron are a type called G-Protein Coupled Receptors and behave predictably when surrounded by more dopamine in that synaptic space. They can be stimulated more easily than in the usual situation where there is not as much dopamine in the synapse.
I’m trying to avoid getting too technical, but the behavior of G-Protein Coupled Receptors (the basis for the Nobel Prize in 2012) explains the rapid improvement that eventually starts to wear off between doses and eventually requires increasing doses to get the desired benefits.
The 1960s explanation of levodopa’s mechanism of action explained the wearing off of benefits and need to increase doses in ways that are incompatible with today’s knowledge. The data indicate that levodopa improves movement in people with Parkinson’s via extracellular effects – not on the presynaptic neuron where excess dopamine is causing toxicity, but rather on the post-synaptic dopamine receptors.
Levodopa vs. RB-190: Is There a Conflict?
Many times, experts have told me that my views and approaches cannot be valid because they contradict each other and accepted knowledge. But that is not so.
The data teach that excess dopamine exists inside the presynaptic neurons, where its metabolism produces toxins that cause dysfunction and death of these vital neurons. The data also teach – as I’ve tried to summarize above – that in Parkinson’s, levodopa acts extracellularly on post-synaptic dopamine receptors and does not meaningfully enter the presynaptic axon. It does not cause toxicity to these presynaptic cells because it does not get inside them. This anatomic division between the sites of action of RB-190 and levodopa is why I do not tell people to stop or avoid levodopa. In that context, remember that while levodopa does not slow or reverse the disease, it can bring meaningful benefits to people with PD.
Our goal is to focus instead on how to reverse the disease. To do so, recognized the data showing that the amount of dopamine inside the presynaptic dopaminergic neurons is excessive, which leads to toxicity that can explain the progression of the disease. And that toxicity was reversed by RB-190 in nine laboratory models of disease. Dopamine-related toxicity in the pre-synaptic neuron appears to drive the disease and is the target of RB-190. Levodopa palliates symptoms via its extracellular, post-synaptic mechanism of action. Both relevant to Parkinson’s while independent in their biologic and clinical effects.
I don't want to appear to be hypercritical. I'm certainly not a negative person. But I learned long ago in the importance of asking questions. By doing so, I learned, and shared with you today, that while the data teaches that levodopa is useful to manage symptoms, RB-190 could powerfully reverse the underlying disease.
Share This
|
Sign up at: ParkinsonsDisease.blog |
About Jonathan Sackner-Bernstein, MD
Dr. Sackner-Bernstein shares his pursuit of conquering Parkinson's, using expertise developed as Columbia University faculty, FDA senior official, DARPA insider and witness to the toll of PD.
Dr. S-B’s Linkedin page
RightBrainBio, Inc. was incorporated in 2022 to develop tranformative therapies for people with Parkinson's.